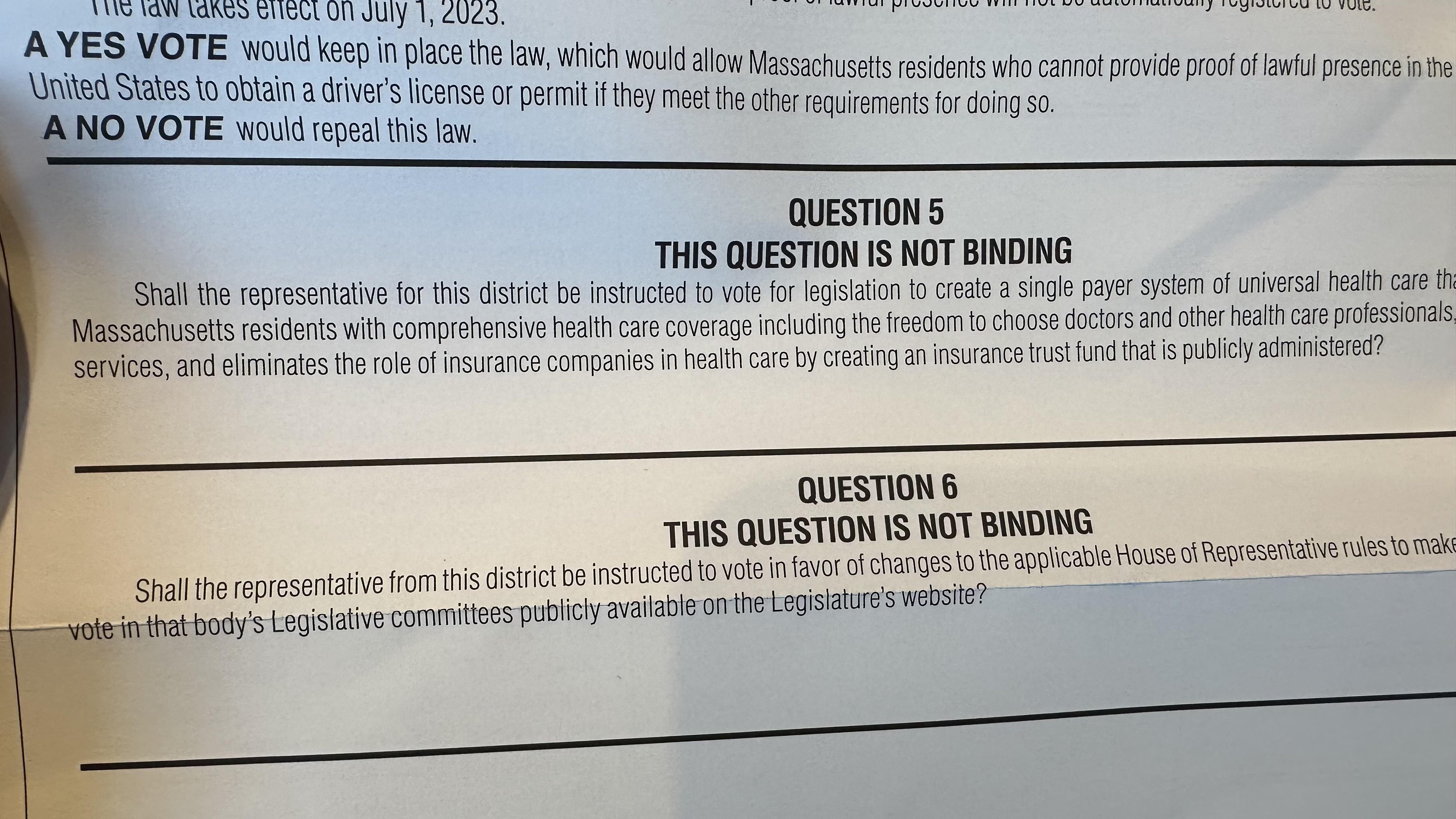
 Questions 5 and 6 seem like a no brainer to me. Anyone want to try and change my mind?
Questions 5 and 6 seem like a no brainer to me. Anyone want to try and change my mind?Submitted by MarcoVinicius t3_yaydhd in boston
man2010 t1_itg7pmh wrote
Reply to comment by Angri_1999 in Questions 5 and 6 seem like a no brainer to me. Anyone want to try and change my mind? by MarcoVinicius
A one year record surplus isn't a sustainable funding source for single payer healthcare
Angri_1999 t1_itgd77q wrote
I don’t know if the proposed non-biding question is the -right- use of the funds, but we’re run a surplus and re-built the rainy day over the last few years. Surely there are places that could use the funds. (Not meaning to attack, I just have a reflex response to “we can’t pay for it” when we had a tax refund)
The current wait time at DDS (disability services) to have your application reviewed by someone with the appropriate medical degree is over a year. Your medical releases will expire before the person who is tasked with it gets around to calling providers. Perhaps we could hire more reviewers?
Similarly, the DDS reimbursement rate for PCA’s (personal care assistants) to help disabled people with everyday life tasks is currently less than $20/hr. Even if you’re approved for a specified number of hours of care, the reimbursement rate is too low to get the care you need. A proposed budget amendment earlier in the year included raising the rate to $20, but it’s sponsor was convinced to remove it.
We could revise the chapter 70 formula to send more money back to schools (especially those with low income students, ELLs, and disabled students - places where we know the foundational level doesn’t match the actual cost to educate)
We could actually staff MBTA maintenance to the levels recommended in the FTA report (we’re currently at either 80%, or 60% if you don’t use mandatory overtime, of the number of workers needed to maintain the system)
I’m pretty sure every department that has a secretary (Education, Transportation, etc.) has unmet needs. Let’s fund some of those.
man2010 t1_itgqfcc wrote
A lot of these aren't really comparable to implementing single payer healthcare at the state level since they're either one time costs that make sense to use our one time record surplus on or aren't at all comparable in terms of cost to single payer healthcare. Our one year surplus isn't useful when talking about a new, massive public health program that would need to be funded in perpetuity.
Viewing a single comment thread. View all comments