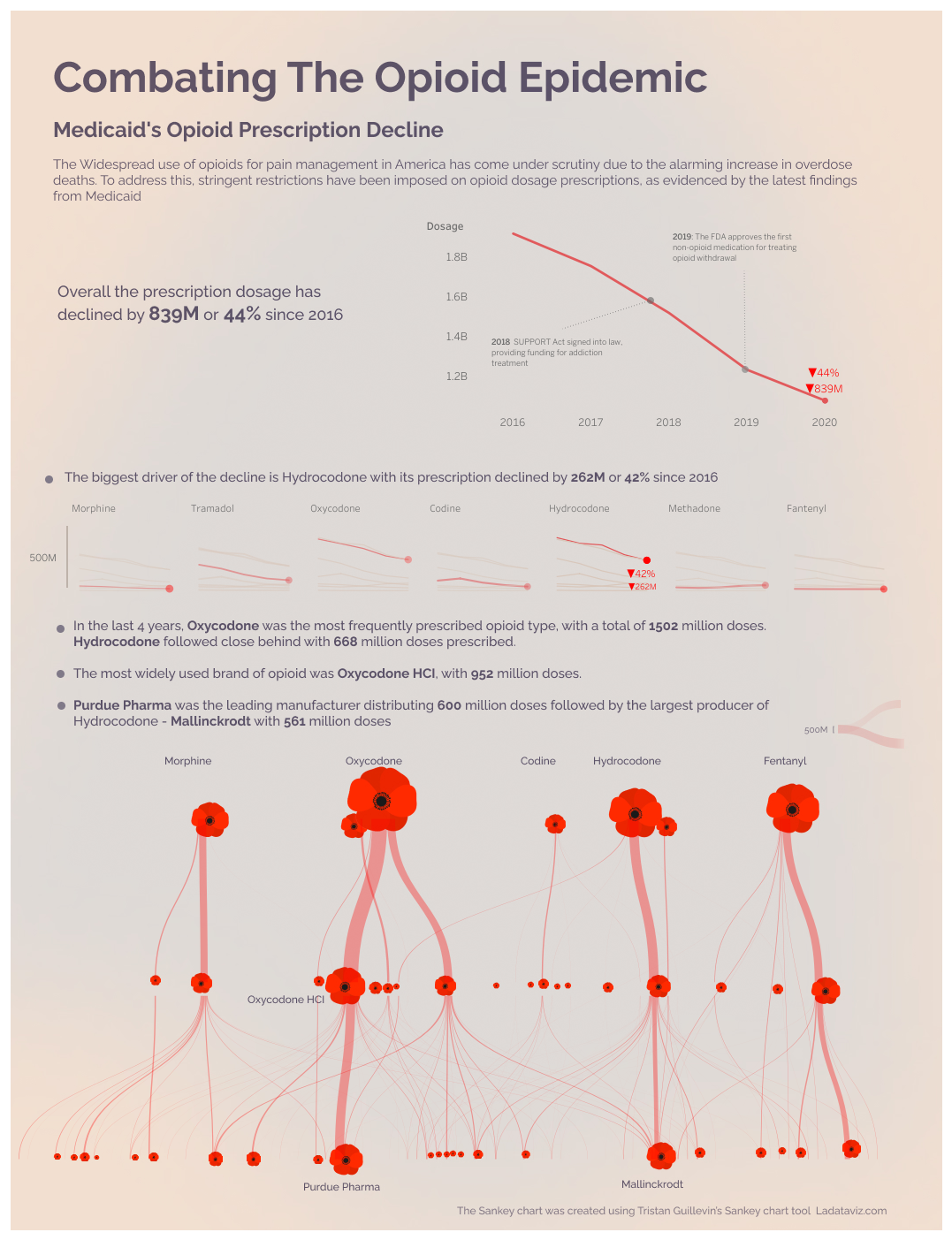
 [OC]Combating The Opioid Epidemic Medicaid's Opioid Prescription Decline
[OC]Combating The Opioid Epidemic Medicaid's Opioid Prescription DeclineSubmitted by Away-Pepper-9239 t3_11056fr in dataisbeautiful
Alternative-Sea-6238 t1_j88lnu6 wrote
Reply to comment by designer_of_drugs in [OC]Combating The Opioid Epidemic Medicaid's Opioid Prescription Decline by Away-Pepper-9239
Firstly my post was simply a list of analgesics. That was what was asked for.
Secondly you may think that. And you are obviously entitled to your opinion. Your opinion is not seemingly well based in fact. Or perhaps maybe your reply is by someone who who doesn't know about outpatient or chronic pain use. I don't know.
I mention paracetamol, naproxen, ibuprofen, diclofenac, gabapentin, pregabalin, duloxetine, magnesium, local anaesthetics, heath and cold therapies, all of which are available and appropriate for some outpatient or chronic use. So basically the majority of what I listed.
designer_of_drugs t1_j88m0xx wrote
You made a list of drugs that are not practical for most situations. It gives a totally misleading picture of the state of pain management as is related to opioid replacement.
Alternative-Sea-6238 t1_j88nup7 wrote
I made a list of drugs for pain relief as that was what was asked for. There are very few situations (arguably none) in which all drugs are practical.
Expecting any drug to replace opioid is very unrealistic at this time and as I have commented on, dealing with chronic pains should be multidisciplinary and not entirely reliant on just pharmaceutical therapy for the most effective way of tackling the issue.
One of the largest barriers is tackling patient (and indeed many healthcare provider) mindsets and psychologies. Opioid rotation is not a long term solution. Opioid reduction is the main aim but requires a huge turnaround of thinking/effort/money.
Prevention is better than cure generally. Stopping the opioid problem in a patient beforenit deveoops into a massive chronic issue is far better than trying to sort it when they aren on 160mg BD and it's five years down the line. One situation that can be worked on is the acute pain apatient who comes to hospital (e.g. After a trauma). If the analgesia is effectively tackled then, with the likes of the medications I have mentioned, and they get discharged without the need for ever escalating opioid prescriptions, how is that a bad thing? If you disagree and you think they should just get ever escalating doses of single agents then, again, that's your opinion.
As of yet there is no panacea and I doubt there ever will be. Based on your name I'm guessing that you are somehow involved in the pharmaceutical industry? If this is the case then no doubt you are aware of how difficult it is to create a drug that has decent efficacy, acceptable tolerance and safety profile and a cost efficient process of manufacturing, distribution and marketing.
I never said
Viewing a single comment thread. View all comments