joxeloj
joxeloj t1_jeewatt wrote
Reply to comment by CaptainHindsight92 in Sublingual Spray With THC And CBD Can Control Blood Sugar, Lowers Cholesterol In Type 2 Diabetes Patients by Defiant_Race_7544
I actually work in neuroscience/psychiatry research and I do not see this "weed-fixes-all" research. I am very open to the idea of cannabis being effective for many medical indications but the evidence isn't there, and plenty of it is negative. Are you sure you're not mistaking overstated in vitro work and medical hypotheses-level reviews posted on this subreddit by mouth breathers, with actual evidence for efficacy in medical illness is humans?
This is a phase I double-blind, randomized controlled trial. This is fairly strong in-human evidence. As it stands there is evidence from observational studies that obesity is less common among chronic, frequent cannabis users so a metabolic effect like this would not be unprecedented per se.
joxeloj t1_jbrjaht wrote
Reply to comment by merchant_of_mirrors in Ancient dormant viruses found in permafrost, once revived, can infect amoeba. Findings hint at a much bigger problem—as the planet warms and the permafrost melts, there is a chance of viruses emerging that are capable of infecting humans by Wagamaga
Bacteria is not news, human pathogenic viruses are, and it's a very different scenario. There are absolutely levels of risk and viruses are not bacterial spores.
joxeloj t1_jbqwlcb wrote
Reply to Ancient dormant viruses found in permafrost, once revived, can infect amoeba. Findings hint at a much bigger problem—as the planet warms and the permafrost melts, there is a chance of viruses emerging that are capable of infecting humans by Wagamaga
I'm EXTREMELY skeptical this is a meaningful risk. Viruses infecting single cell organisms are extremely abundant in the environment but do not pose a threat to humans.
Viruses that infect humans or even mammals immensely less abundant, so very few if any will stand a chance of being preserved in this manner. It seems astronomically unlikely they would then make it back into a living host in sufficient numbers while still viable to achieve a productive infection. I imagine an infected carcass would have to freeze very quickly for viable viruses to be preserved, and then be consumed in large amounts fairly quickly to infect something.
Even if they did, they'd be less likely to achieve subsequent transmission relative to current viruses in active circulation and no more likely to be lethal/highly pathogenic. This just reads like a scary sentence you put at the ending of a basic microbiology paper to garner media coverage and win career points.
joxeloj t1_jbq9hij wrote
Reply to comment by That-Group-7347 in Comprehensive review and trial results of upcoming antidepressant Ruoxinlin (ansofaxine) by That-Group-7347
Citation? Because if you're referencing that amphetamine challenge paper you are way off the mark. We have definitely had methods to image extracellular serotonin via radio-labelled serotonin receptor ligands for decades.
joxeloj t1_j926kd1 wrote
Reply to comment by Tight-Caterpillar-25 in Psychedelics activate the same receptors as serotonin, so why aren't we always tripping? Psychedelics may cause neuronal plasticity and relieve depression by activating intracellular serotonin receptors that serotonin itself cannot, suggests a new study. by rjmsci
MDA has mild psychedelic effects, because it has some agonist activity at 5-HT2A receptors. If you take enough MDMA occasionally those effects can bleed through towards the tail end of the roll. Very mild visuals at most. Related drugs like 5-MAPB are pure empathogens without psychedelic effects. Methamphetamine at high doses has empathogen effects without psychedelic effects as well. Serotonin release does not induce psychedelic effects. Phenethylamine 5-HT2A agonists can.
Empathogenic effects arise from serotonin release and involve a sense of profound empathy for oneself and others, desire to socialize, anxiety reduction, euphoria, etc while remaining relatively cognitively intact and without meaningful changes in visual perception. These drugs are usually stimulating to some extent. Psychedelic effects arise from biased 5-HT2A agonism and involve vivid, colorful visual hallucinations composed of repeating patterns, loss of sense of self, thought loops, etc without implicit euphoria or anxiolytic effects and in many cases without stimulating effects. Very different experiences.
joxeloj t1_j91oxkx wrote
Reply to comment by Tight-Caterpillar-25 in Psychedelics activate the same receptors as serotonin, so why aren't we always tripping? Psychedelics may cause neuronal plasticity and relieve depression by activating intracellular serotonin receptors that serotonin itself cannot, suggests a new study. by rjmsci
Have you ever done any of these drugs? Metabolic conversion to MDA (which has some 5-HT2A agonist properties) can create some extremely minor psychedelic effects towards the end of the roll as serotonin levels fall but it's not in the same ballpark as any legitimate psychedelic. There's a reason the empathogen/enactogen classification was created.
joxeloj t1_j8zfd9h wrote
Reply to comment by Tight-Caterpillar-25 in Psychedelics activate the same receptors as serotonin, so why aren't we always tripping? Psychedelics may cause neuronal plasticity and relieve depression by activating intracellular serotonin receptors that serotonin itself cannot, suggests a new study. by rjmsci
Serotonin releasing agents are not psychedelic hallucinogens, and hallucinations that might occur during serotonin syndrome are most likely true hallucinations, not psychedelic hallucinations.
joxeloj t1_j8kxao3 wrote
Reply to For those interested in communal/common mycorrhizal networks (e.g., Finding the Mother Tree) - Positive citation bias and overinterpreted results lead to misinformation on common mycorrhizal networks in forests Nature Ecology & Evolution by Propeller3
Seems to be a common thread among the bulk of scientists in this field. I took an interest in this as a neuroscientist and watched some conference presentations because the lay media poorly presented. Amusingly, most people took time to subtly throw shade at people like Simard.
joxeloj t1_j8gktry wrote
Reply to comment by l4mbch0ps in Children as young as 4 years old show evidence of a network in the brain found in adults that tackles difficult cognitive problems, a new fMRI study found. Researchers were surprised, thinking it may take longer for the multiple demand network to differentiate in humans. by geoff199
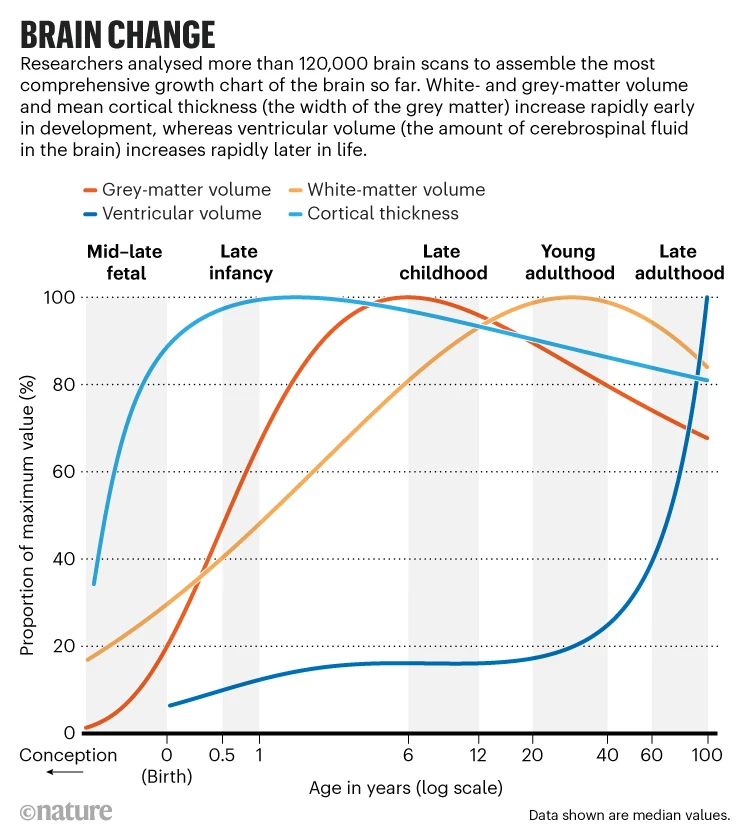
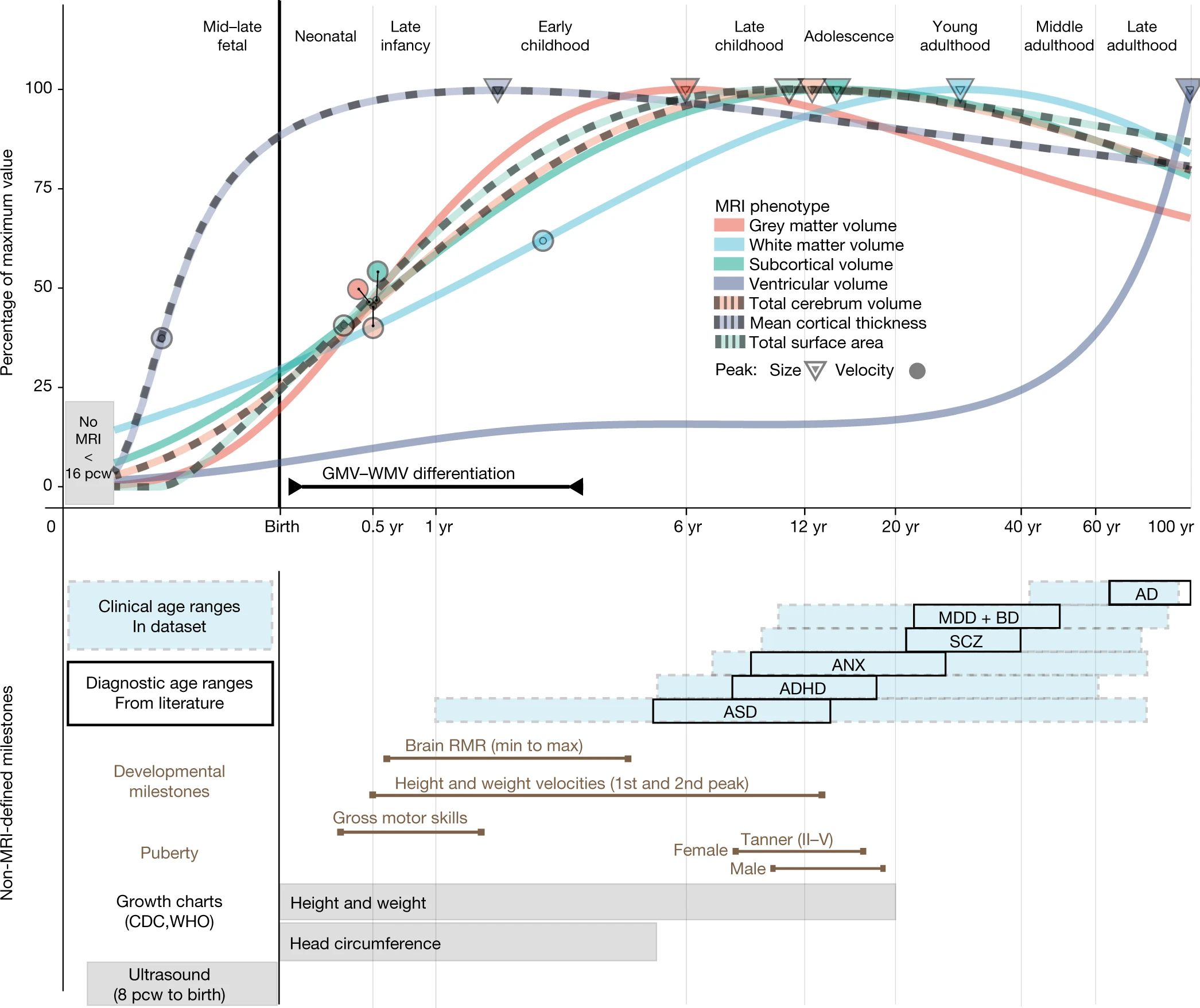
Kids are dumb but 25 is a pop sci meme based on extremely low levels of asymptotic but non-zero synaptic pruning and white development in the PFC not tied to any cognitive functions or behavioral changes. By 16 the vast majority of brain development is done and adult-level cognitive function is reached. By 18 you get adult-level psychosocial maturity. In the most extreme stretch of the data the latest I would say the brain is still meaningfully developing is 20 but I would personally draw the line at 18.
This is absolutely not the sole study I'm basing this on (it's consistent with decades of data), but if you want to read more here is a nice lay article about recent work characterizing brain development over the lifespan, and a nice summary figure. Here is the paper being summarized, which is somewhat approachable itself, with figure 3 being the most important summary figure. Note the general ideas are pretty consistent 20+ year old models of brain development
{kind=link}
{kind=link}
{kind=link}
joxeloj t1_j6pcadn wrote
Reply to comment by dizzariffic in Canada province decriminalizes hard drugs in new bid to combat opioid crisis by scot816
Compulsory treatment is objectively ineffective and only serves to further a moral crusade against drug use. The vast majority of the social, economic, and health consequences of which arise from its stigmatization and a lack of regulation.
Even voluntary, motivated treatment has much poorer effectiveness than the vast majority of people seem to believe. The most effective treatment for opioid addiction, the global gold standard, is literally giving the individual stable daily doses of opioids to take in place of street opioids. The most effective opioid replacement therapies in terms of quality of life, socioeconomic functioning, and health outcome/preventing deaths are literally the more recreational opiates; buprenorphine < methadone < oral morphine < injectable hydromorphone.
joxeloj t1_jegaunh wrote
Reply to comment by SaltZookeepergame691 in Sublingual Spray With THC And CBD Can Control Blood Sugar, Lowers Cholesterol In Type 2 Diabetes Patients by Defiant_Race_7544
You're correct that many of the p-values are off. Even some of their Fisher Exact tests are off (e.g. I get p=0.47 for hypertension). I think they probably used Mann-Whitney U tests after a Shapiro-Wilk's p<0.05 for many of these, but I can't prove that without access to their data. It is odd overall.
I will point out they claim to test their primary hypothesis by ANCOVA accounting for baseline values, and randomization is not necessarily pointless even if you don't end up with well-balanced groups by specific endpoints. With that said you could probably get a response published on the basis of some of these discrepancies.